I have spent the better part of three decades watching epilepsy behave differently depending on where patients live. Early in my career, when I was building the Texas Comprehensive Epilepsy Program at UTHealth Houston, I noticed something that every neurologist in the South quietly understands but rarely says out loud: the patients arriving from East Texas, from rural Louisiana, from the Gulf Coast corridor were arriving later, sicker, and with fewer resources than patients from virtually anywhere else in the country. They had often waited years for a diagnosis. Many had never seen a specialist. Some had never held a job because their seizures were uncontrolled, not because treatment had failed — but because treatment had never really begun.
I did not have the data to prove it then. Now, thanks to a landmark study just published in JAMA Neurology, we do.
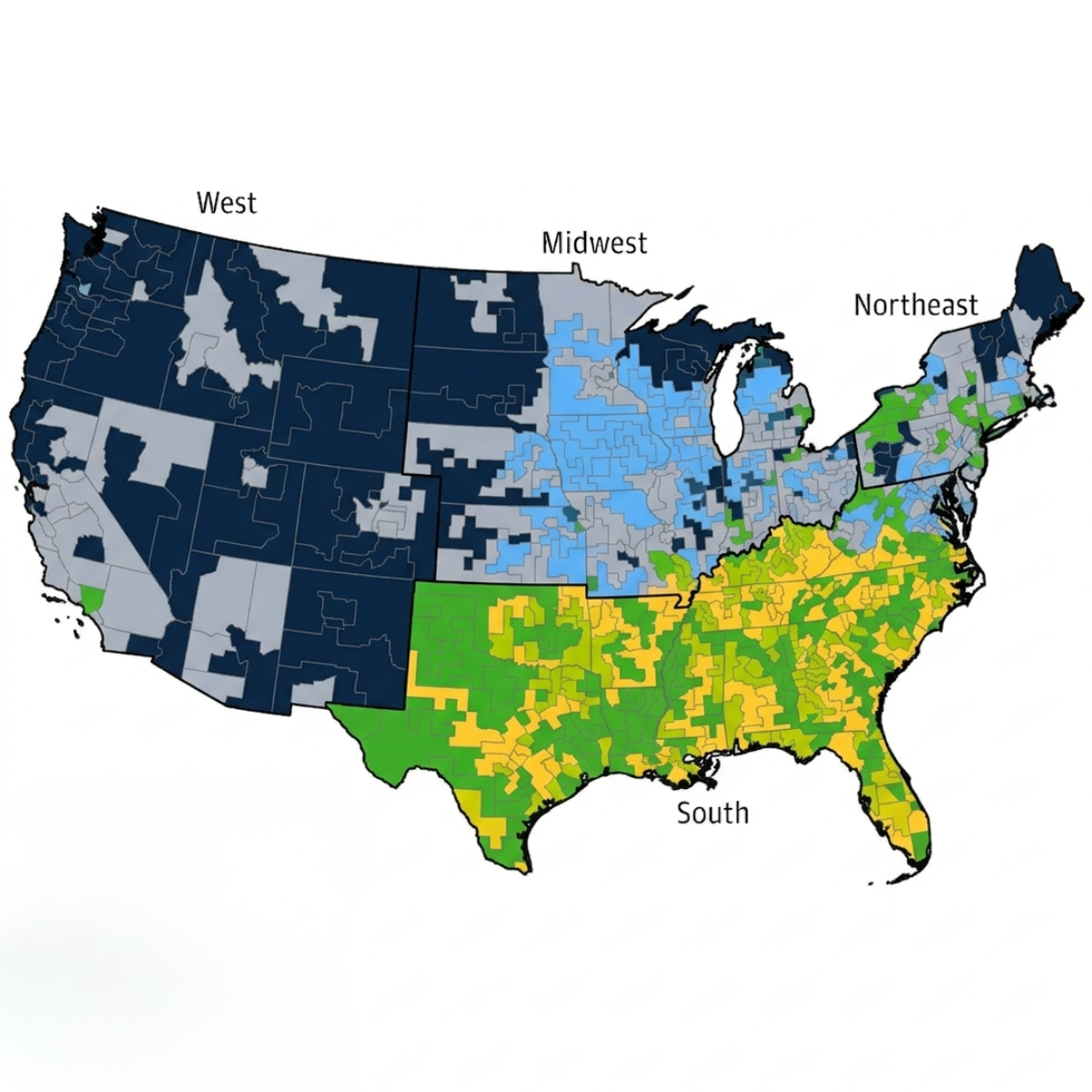
Researchers at Case Western Reserve University, led by Dr. Weichuan Dong and colleagues, have produced the most geographically granular map of epilepsy incidence among older Americans ever assembled. Drawing on Medicare claims data for nearly five million beneficiaries aged 65 and older, and applying an innovative spatial methodology called Max-P regionalization to preserve patient privacy while achieving county-level precision, their team identified more than 20,000 incident epilepsy cases in 2019. What they found should command the attention of every neurologist, public health official, and health system leader in the United States: epilepsy incidence among older adults varies more than tenfold across American geography — from 141 per 100,000 in parts of western Iowa to 1,476 per 100,000 in coastal South Carolina — and the highest-burden regions cluster unmistakably in the American South.
Louisiana. Eastern Texas. Central Oklahoma. The Appalachian corridor of Kentucky and West Virginia. These are not random data points. They are a pattern — one the authors explicitly compare to the Stroke Belt, the well-known band of elevated stroke mortality that has shadowed the same geography for decades. They call it, appropriately, the Epilepsy Belt.
I would know. I worked inside it.
What the Data Actually Show and Why It Matters
The study's methodology deserves a moment of appreciation before we discuss implications. Traditional county-level analyses of epilepsy have been hamstrung by a fundamental problem: in most counties, there simply aren't enough cases to calculate a statistically reliable incidence rate.Nearly 88 percent of US counties in this dataset had fewer than 11 incident cases — too few to report under Medicare confidentiality rules. Previous attempts at geographic mapping of epilepsy have either been forced to the state level (too coarse to be actionable) or limited to small regional datasets.
The Max-P regionalization approach solves this elegantly. It aggregates neighboring counties with similar socioeconomic profiles — using the Area Deprivation Index as a guide — until each resulting "MaxCounty" meets the minimum case threshold. The result is 692 spatially coherent regions that preserve geographic meaning while enabling rigorous statistical analysis. It is the kind of methodological innovation that opens a door previously locked.
Once that door opened, the findings poured through.
The highest epilepsy incidence is not distributed randomly. It is a heat map of disadvantage. The authors used both random forest machine learning and logistic regression to identify which community-level factors predicted high-incidence areas, and the results tell a coherent story about the social infrastructure — or rather the absence of it — that surrounds older adults in these regions.
Insufficient sleep was the single most powerful predictor. Communities where large proportions of adults sleep less than seven hours per night had nearly double the odds of being high-incidence epilepsy regions. This makes clinical sense on multiple levels. Sleep deprivation is a well-established seizure trigger, lowering seizure threshold in people already predisposed to epileptic activity. But the authors make a deeper point: in older adults, insufficient sleep is itself embedded in poverty. Chronic financial stress, physical discomfort from inadequate housing, noise, unsafe neighborhoods, multiple jobs — all of these erode sleep, and all of them are concentrated in the same geography where epilepsy is highest.
Extreme heat was the second most powerful predictor. The Southern states that anchor the Epilepsy Belt are also the states where days with a maximum heat index above 95°F are most frequent. Heat stress disrupts sleep, affects vascular function, and alters the pharmacokinetics of antiseizure medications — a convergence that plausibly raises seizure risk in already-vulnerable older adults. As climate change drives more extreme heat events across the South, this association carries a warning that will only grow louder.
Lack of household vehicle access had an odds ration early identical to that of insufficient sleep — communities in the highest tertile for car-free households had 93 percent greater odds of being high-incidence regions. In rural and semi-rural parts of the South, not having a car is not an inconvenience. It is a catastrophic barrier to healthcare. It means missed follow-up appointments. It means prescriptions not picked up. It means the first seizure that should have triggered a neurology referral instead triggers an emergency room visit eighteen months later, when the condition has solidified into chronic epilepsy.
Insurance gaps told a story I have lived. The study found that uninsurance rates among adults aged 18 to 64 were highest in Texas, Florida, and Georgia — states that have also resisted Medicaid expansion — and these same states showed elevated epilepsy incidence in the older Medicare population. This is a critical temporal insight. The authors suggest that reduced healthcare access or delayed diagnosis at younger ages may propagate into higher epilepsy rates in the elderly. Epilepsy is not a condition that waits patiently for coverage to begin at age 65. Missed diagnoses, undertreated seizures, and accumulating neurological injury over decades of uninsurance all arrive in the Medicare system as a more severe disease burden.
Texas: A Case Study in Structural Vulnerability
I want to dwell on Texas specifically, because I know this state, its patients, and its healthcare landscape in ways that go beyond the published data.
Texas has the highest uninsured rate in the country. It has not expanded Medicaid. It has vast rural geographies with sparse neurology coverage, where patients routinely drive three or four hours each way to reach a comprehensive epilepsy center. Its eastern counties — the ones that show up dark red on the study's incidence map — sit squarely in the region that overlaps with both the Stroke Belt and now the Epilepsy Belt. They are also among the most socioeconomically disadvantaged counties in the United States.
When I ran the Texas Comprehensive Epilepsy Program, we saw the consequences of this system every day. Patients who had been on phenytoin for twenty years because nobody had ever offered them a newer medication. Patients whose seizures were uncontrolled because the generic version of their antiseizure medication had been substituted at the pharmacy without a physician's knowledge. Patients who qualified for epilepsy surgery evaluations but could not access them because the evaluation required multiple extended hospitalizations, and they could not afford the time off work or the travel. Patients who had lost their driver's licenses — the only practical means of transportation in rural Texas — creating a vicious cycle in which the seizure condition that required care also eliminated the ability to seek care.
The new JAMA Neurology data confirm what those of us who practiced in this region already suspected. But confirmation matters. It transforms clinical intuition into evidence, and evidence is what moves policy.
The Stroke Belt Connection
The authors make a point worth emphasizing: the EpilepsyBelt and the Stroke Belt are not coincidentally co-located. They are, in large part, the same phenomenon.
Stroke is the most common identifiable cause of epilepsy in older adults. It accounts for roughly one-third of new-onset seizures after age 65. The southeastern United States has had elevated stroke mortality for solong that researchers have been studying it for decades, tracing it to aconvergence of hypertension, diabetes, obesity, socioeconomic stress, healthcare access barriers, and racial health disparities. All of those sameforces appear in the epilepsy data.
This means that a significant fraction of the "Epilepsy Belt" may represent, at its mechanistic core, the late neurological consequences of the Stroke Belt — the seizure disorders that arise from infarcted brain tissue in populations where strokes happen more often, are more severe, and are treated less effectively than in other parts of the country.
This reframes prevention in an important way. Reducing stroke incidence and improving acute stroke care in the South is not just a cardiovascular intervention. It is a neurology intervention. It is an epilepsy intervention. The diseases do not respect specialty boundaries, and neither should our public health response.
The Protective Factors Deserve Attention Too
The study did not only find risk factors. It also identified two community characteristics associated with lower epilepsy incidence, and they are worth pondering.
Higher employment in agriculture or natural resources was associated with a markedly lower likelihood of high epilepsy incidence — an odds ratio of 0.37, meaning roughly a 63 percent lower probability. The authors suggest this may proxy for lower population density, lower stress, or healthier lifestyle patterns associated with physical outdoor work. There is emerging evidence from Japan and elsewhere that regular agricultural activity is associated with better chronic disease control. Whatever the mechanism, these are communities worth studying more carefully for what they may be doing right.
Higher rates of recent in-migration from other states were similarly protective. The authors invoke the "healthy migrant effect" — the well-documented phenomenon in which people who migrate tend to be healthier than those who stay, at least initially. Communities with active in-migration may also be more economically dynamic, with better employment opportunities and less concentrated deprivation. Both protective factors were most prevalent in the lower-incidence regions of the Great Plains and Mountain West — geographies that appear, in multiple ways, to be doing better by their older populations.
What Needs to Happen
This study is a diagnosis. What is the treatment?
Sleep health must be taken seriously as a public health priority. This sounds deceptively simple. It is not. Addressing population-level insufficient sleep requires addressing the poverty, housing instability, chronic stress, and neighborhood conditions that rob people of rest. But it also means that clinicians in high-incidence regions should be screening for sleep disorders more aggressively, because sleep apnea in particular is both common in older adults and a modifiable contributor to seizure risk.
Transportation barriers require structural solutions. Telehealth expanded enormously during the COVID-19 pandemic, and epilepsy care was among the specialties that benefited. Patients who could not drive to clinic could finally access their neurologist remotely. Additionally, in-home EEG testing brings diagnostic testing that these patients need right to their doorstep. Policies that preserve and expand telehealth coverage and in-home testing for epilepsy, particularly in rural and transportation-disadvantaged communities, are a direct response to one of this study's most striking findings.
Medicaid expansion in holdout states is a neurology issue. This is not a political argument. It is a medical one. The data show that states with the highest uninsurance rates in working-age adults have the highest epilepsy incidence in older adults. The pipeline from uninsured young adult to undertreated elderly patient with new-onset seizures is real and measurable. Closing that coverage gap is one of the highest-yield structural interventions available.
Heat resilience infrastructure matters for neurological health. Cooling centers, urban tree canopy, and housing improvements that reduce indoor heat exposure are not traditionally thought of as neurology interventions. They should be — particularly in the communities this study has now mapped with precision.
Health systems in high-incidence regions need to invest in EEG capacity and epilepsy monitoring infrastructure. One of the things I have come to understand through my current work operating across hundreds of hospital systems nationally, including many in the regions identified by this study, is that the gap between seizure occurrence and proper diagnosis is often a technology and capacity problem. Hospitals in high-incidence areas frequently lack sufficient EEG monitoring capability to properly evaluate, classify, and manage new-onset epilepsy in older adults. The patients are there. The disease is there. The diagnostic infrastructure is often not.
This is where Stratus can step in and help. I joined Stratus as their Chief Medical Officer because I saw the need for high-quality, ambulatory EEG testing. With many rural hospitals not able to staff a full time EEG technician, never mind have a qualified EEG Technologist to monitor patients in an EMU setting, outsourcing a diagnostic EEG test to Stratus is a win for both the hospital and the patient.
A Map Is Not Enough
I want to close with something that I feel deeply, after three-plus decades in this specialty.
Maps of disease burden are powerful. They focus attention. They guide resource allocation. They give us language — "EpilepsyBelt" — that can make a complex health disparity concrete enough to hold in the mind and argue about in a policy meeting. The JAMA Neurology paper has done something genuinely valuable in producing a cleaner geographic picture of epilepsy in older Americans than has ever existed before.
But maps are not enough. The communities with the highest epilepsy incidence in this study are the same communities that have been identified as disadvantaged in study after study, decade after decade. They are concentrated in the same states, many of which have made conscious political decisions to limit Medicaid expansion, resist healthcare infrastructure investment, and underfund public health. The data keep arriving. The geography barely moves.
The epilepsy patients I treated in East Texas were not statistics. They were people who had worked hard, often in physically demanding jobs, in a hot and humid climate, without adequate sleep, without always having health insurance, sometimes without a car, trying to manage a neurological condition that most people around them did not understand. They deserved better than the system they had. Most of them still do.
What this study demands is not just acknowledgment but commitment: to use these data to drive targeted investment in the communities they identify, to advocate for the structural changes — insurance coverage, transportation access, heat resilience, sleep health — that will actually move the needle, and to ensure that the diagnostic and treatment capacity of health systems in the Epilepsy Belt is commensurate with the burden they carry.
The map is drawn. Now we need the will to act on it.
Reference: Dong W, Cabulong A, Vu L, et al. Incidence and Risk Factors of Epilepsy Among Older Adults in the US Medicare Population. JAMANeurology. 2026;83(2):161–170. doi:10.1001/jamaneurol.2025.4347
About the Author
About the Presenter

Jeremy D. Slater, MD, FAAN, FAES, FACNS
Jeremy D. Slater, MD, FAAN, FAES, FACNS is a board-certified neurologist and Chief Medical Officer at Stratus. As former Director of the Texas Comprehensive Epilepsy Program at UTHealth Houston, Dr. Slater has specialized in epilepsy and clinical neurophysiology for over 35 years. His extensive background in academic research and clinical practice informs his current focus on expanding the reach of EEG technology and remote neurodiagnostic services. Dr. Slater is a frequent contributor to medical literature and a leading voice in the integration of digital health and neurology. Explore his full publication history via Google Scholar and ORCID.



.svg)
%201.svg)